If you’re looking for peptides to help in the bedroom, then this guide will help break down all the latest from peptide therapy that effect libido for both men and women.
Most solutions for sexual dysfunction target blood flow.
PDE5 inhibitors like sildenafil work on blood vessels — they don’t touch the brain circuits that drive desire, arousal, or hormonal regulation. That’s why they fail for a significant percentage of users, and why they do nothing for low libido.
Peptides work differently. They target the upstream mechanisms — the brain signaling, the hormone cascades, the neural circuits that initiate sexual response before blood flow even enters the picture. Researchers are studying several peptides that operate through distinct pathways: melanocortin signaling, HPG axis regulation, oxytocin bonding circuits, and pineal-mediated hormone balance.
This guide covers the most studied peptides for sexual health, how they work, what the clinical data shows, and how researchers are stacking them for compounded effects.
All content on this page is for informational and educational purposes only. These compounds are research chemicals. Consult a qualified healthcare professional before considering any peptide compound.
What Are Peptides and How Do They Boost Sexual Wellness?
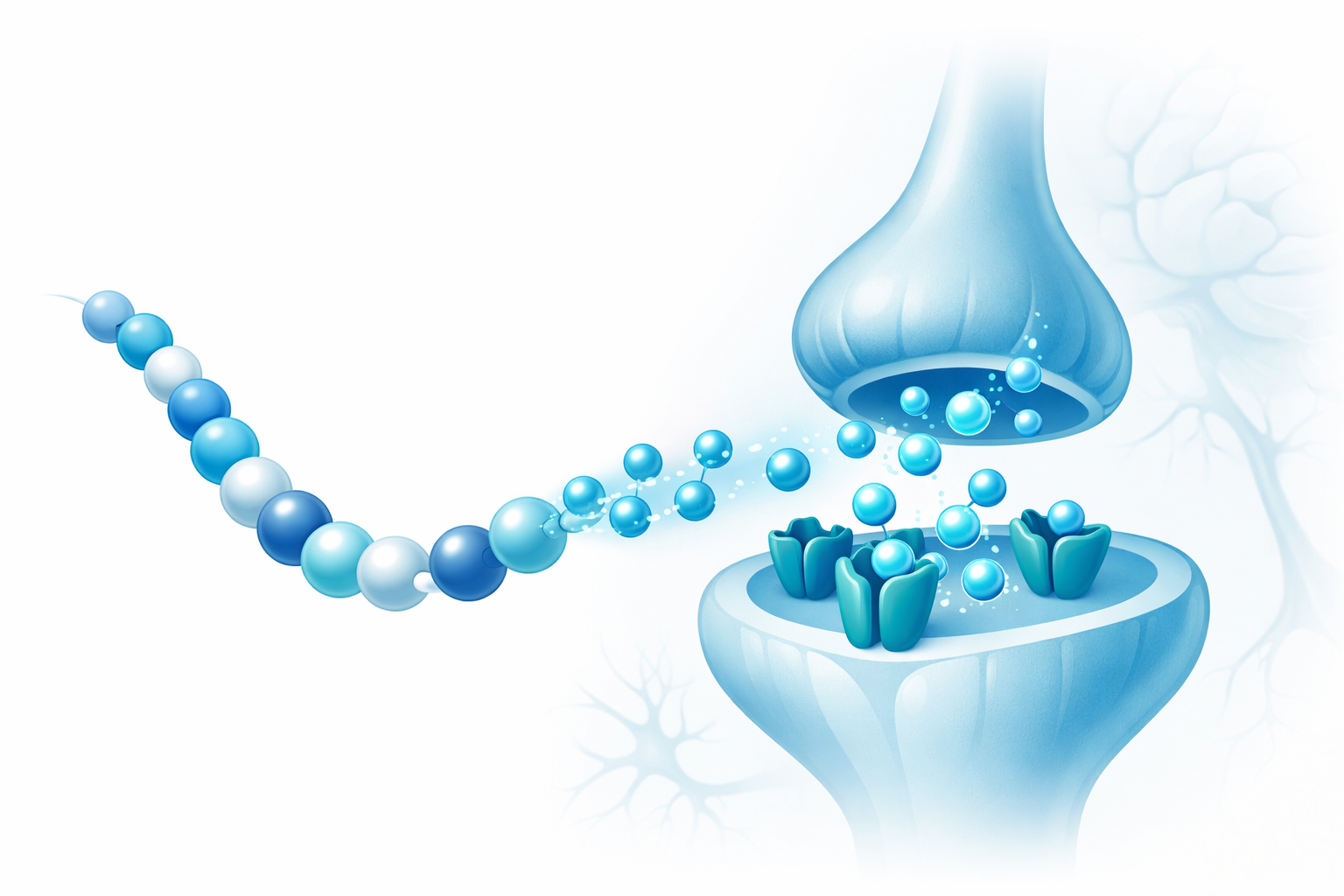
Peptides are short chains of amino acids — typically between 2 and 50 — that act as signaling molecules throughout the body. Unlike pharmaceutical drugs that often target a single receptor with brute force, peptides work through the body’s existing signaling infrastructure. They bind to specific receptors, trigger cascading biological responses, and then break down naturally. If you’re new to peptide research, our complete guide to peptides covers the fundamentals.
For sexual health specifically, peptides target three distinct layers that conventional treatments largely ignore:
- Hormonal axis regulation — The hypothalamic-pituitary-gonadal (HPG) axis governs testosterone, estrogen, LH, and FSH production. Kisspeptin is the master upstream regulator of this entire cascade.
- Central arousal initiation — The hypothalamus and limbic system generate sexual desire through melanocortin signaling and dopaminergic circuits. PT-141 operates here.
- Bonding and intimacy circuits — Oxytocin modulates trust, pair bonding, and the emotional dimension of sexual experience that pure vasodilators cannot address.
- Neuroendocrine balance — Pinealon influences melatonin regulation and stress hormone modulation, indirectly supporting the hormonal environment required for healthy sexual function.
These mechanisms interact but remain distinct. A peptide that increases central arousal (PT-141) works through completely different pathways than one that restores hormonal pulsatility (Kisspeptin). This is why researchers are particularly interested in peptide combinations — stacking compounds that address multiple layers simultaneously.
PT-141: The Top Libido-Boosting Peptide

PT-141 (bremelanotide) is a synthetic melanocortin receptor agonist derived from Melanotan II. It received FDA approval in June 2019 under the brand name Vyleesi for hypoactive sexual desire disorder (HSDD) in premenopausal women — making it the first and only FDA-approved drug that acts centrally on the brain to treat sexual dysfunction.
The compound originated from University of Arizona research on alpha-MSH analogues initially developed for tanning effects. When researchers discovered unexpected pro-sexual effects in male subjects — spontaneous erections without visual or physical stimulation — the research focus shifted entirely. PT-141 was refined from Melanotan II by removing the tanning activity while preserving and enhancing the central sexual arousal mechanisms through structural modification that improved MC4R selectivity.
Unlike PDE5 inhibitors, PT-141 doesn’t primarily affect nitric oxide or cGMP in peripheral vasculature. The arousal response it produces is initiated centrally — brain to spinal cord to peripheral response — rather than peripherally. This distinction is critical because it enables efficacy in PDE5 non-responders and in women, where blood flow isn’t the limiting factor.
Benefits of PT-141 for Men and Women
PT-141 agonizes melanocortin 4 receptors (MC4R) in the hypothalamus and limbic regions — specifically the paraventricular nucleus and medial preoptic area — involved in sexual motivation. MC4R activation drives downstream dopaminergic and oxytocin signaling associated with arousal and motivation.
Clinical evidence in women: The Phase III RECONNECT trials enrolled 1,247 women with HSDD. Both studies showed statistically significant improvements in satisfying sexual events and sexual desire scores versus placebo. These results led directly to FDA approval.
Clinical evidence in men: Phase II trials demonstrated that PT-141 produced erectile response in subjects who had failed sildenafil. A 2004 study by Diamond et al. in the Journal of Sex and Marital Therapy showed erectile response at doses without significant blood pressure effects — a key safety differentiator from vasodilator-based approaches. Reported effects focus on increased sexual desire and arousal rather than simply facilitated erection, which is a mechanistically distinct outcome.
PT-141 Dosage and Administration
In the FDA-approved formulation (Vyleesi), the standard dose is 1.75 mg administered subcutaneously approximately 45 minutes before anticipated sexual activity. Clinical trials established this as the optimal balance between efficacy and tolerability.
Key administration notes from clinical data:
- Onset of action: 30-60 minutes post-injection
- Duration of effect: up to 24 hours in some subjects
- Recommended limit: no more than once every 24 hours
- No more than 8 doses per month (FDA labeling)
- Most common side effect: transient nausea (40% in trials), typically resolving within 2 hours
For proper peptide preparation, review our guide to reconstituting peptides before handling any research compounds.

Kisspeptin: Enhancing Testosterone and Desire
Kisspeptin is a family of neuropeptides encoded by the KISS1 gene, originally identified as a metastasis suppressor before its critical role in reproductive endocrinology was discovered. Peptide forms range from 10 to 54 amino acids (Kp-10, Kp-13, Kp-14, Kp-54), all derived from the same precursor and acting at the same receptor. It is the master upstream regulator of gonadotropin-releasing hormone (GnRH) pulse generation — the switch that controls the entire hormonal cascade.
The human genetics data on Kisspeptin is unusually strong. Loss-of-function mutations in the GPR54/KISS1R receptor cause idiopathic hypogonadotropic hypogonadism (IHH) — individuals fail to progress through puberty and have virtually absent LH, FSH, and sex steroid levels. This confirmed that GPR54 is non-redundant for HPG axis activation. No workaround. No backup system.
How Kisspeptin Improves Sexual Arousal
Kisspeptin’s effects on sexual function operate through two parallel pathways:
Endocrine pathway: Kisspeptin neurons in the arcuate nucleus project to GnRH neurons. Kisspeptin signaling via GPR54 drives pulsatile GnRH release, which drives pulsatile LH and FSH from the pituitary, which drives gonadal sex steroid production. This is the full hormonal cascade — and Kisspeptin sits at the top of it.
Limbic pathway: Kisspeptin neurons also project into the amygdala, hippocampus, and olfactory bulb. A landmark 2017 study published in the New England Journal of Medicine by Dhillo et al. demonstrated that Kisspeptin-54 administration activated limbic and hypothalamic circuits on fMRI, increased penile tumescence, and reduced amygdala activity associated with aversion to sexual stimuli. This was the first evidence that Kisspeptin’s sexual health effects extend beyond hormone production into direct brain circuit modulation.
Kisspeptin for Fertility and Libido
Kisspeptin’s position at the top of the HPG axis makes it uniquely interesting for conditions where the underlying problem is insufficient central drive rather than gonadal failure. A 2009 study by Jayasena et al. showed that repeated Kisspeptin administration restored LH pulsatility in women with hypothalamic amenorrhea — a condition where stress, weight loss, or overtraining has suppressed the hormonal axis.
The mechanistic rationale — restoring upstream drive rather than bypassing the axis with exogenous testosterone — generates significant clinical research interest. Instead of replacing hormones from the outside, Kisspeptin potentially restarts the body’s own production machinery. Research in male hypogonadotropic hypogonadism is ongoing with similar logic.
Kisspeptin also integrates sex steroid negative feedback. It’s the regulatory node that coordinates feedback between gonadal output and central drive — the thermostat of the axis. Estrogen and testosterone suppress Kisspeptin neuron activity, reducing GnRH pulsatility. This makes Kisspeptin research particularly relevant for understanding age-related hormonal decline.
Oxytocin: The Bonding and Intimacy Peptide
Oxytocin is a nine-amino-acid neuropeptide produced in the hypothalamus and released by the posterior pituitary. While widely known as the “bonding hormone” for its role in childbirth and lactation, research over the past two decades has revealed extensive involvement in sexual arousal, orgasm, pair bonding, trust, and social cognition.
In the context of sexual health, oxytocin operates in a fundamentally different domain than PT-141 or Kisspeptin. Where PT-141 drives desire and Kisspeptin regulates hormonal production, oxytocin modulates the emotional and relational dimensions of sexual experience — the components that determine sexual satisfaction beyond physical mechanics.
Oxytocin Benefits for Sexual Health
Research has identified several mechanisms through which oxytocin influences sexual function:
- Orgasm intensity: Plasma oxytocin levels surge during orgasm in both men and women. Studies by Carmichael et al. demonstrated a direct correlation between oxytocin levels and subjective orgasm intensity. Intranasal oxytocin administration has shown enhanced orgasmic function in preliminary trials.
- Erectile function: Oxytocin receptors are present in penile tissue. Central oxytocin release activates spinal cord pathways involved in erection through a mechanism independent of both the NO/cGMP pathway (PDE5 inhibitors) and the melanocortin pathway (PT-141).
- Pair bonding and trust: Oxytocin strengthens partner preference and emotional connection during intimate contact. Research by Scheele et al. showed that oxytocin increased the rewarding quality of a partner’s face in fMRI studies — the brain literally responds more positively to a partner under oxytocin influence.
- Anxiety reduction: Sexual dysfunction frequently co-occurs with performance anxiety. Oxytocin’s anxiolytic effects in social contexts may address this psychological barrier that purely physiological interventions miss entirely.
The most common research administration route is intranasal, with doses typically ranging from 20-40 IU in clinical studies. Effects onset within 30-60 minutes of intranasal administration.

Pinealon: Hormone Balance for Better Sex Drive
Pinealon is a tripeptide (Glu-Asp-Arg) that crosses the blood-brain barrier and targets the pineal gland and neuroendocrine system. Developed through research by the St. Petersburg Institute of Bioregulation and Gerontology, Pinealon belongs to a class of bioregulatory peptides designed to restore function in specific tissue types.
Its connection to sexual health is indirect but mechanistically relevant. Pinealon influences melatonin synthesis and circadian rhythm regulation — and disrupted circadian rhythms directly suppress testosterone production, LH pulsatility, and sexual desire. Chronic sleep disruption reduces testosterone by 10-15% in clinical studies, with corresponding decreases in libido.
Pinealon’s documented effects relevant to sexual health include:
- Melatonin regulation: Normalizing melatonin production supports the circadian testosterone rhythm — testosterone peaks during sleep and requires intact circadian signaling
- Cortisol modulation: Chronic elevated cortisol directly suppresses GnRH (the same pathway Kisspeptin activates). Pinealon’s stress-modulating properties may remove this hormonal brake
- Neuroprotective effects: Protection of hypothalamic and pineal tissue function supports long-term neuroendocrine health
Pinealon is not a direct sexual health peptide in the way PT-141 is. It’s a support compound — one that addresses the environmental and hormonal conditions required for the other peptides and the body’s own systems to function optimally.
Peptide Stacks for Sexual Performance
Because these peptides operate through distinct mechanisms, researchers are investigating combinations that address multiple layers of sexual function simultaneously. The logic is straightforward: stacking compounds that work through independent pathways should produce additive or synergistic effects without compounding side effects from the same mechanism.
PT-141 + Kisspeptin — Desire + Hormonal Drive: PT-141 activates central arousal through melanocortin signaling while Kisspeptin optimizes the hormonal environment through HPG axis regulation. One drives the brain’s desire circuitry, the other ensures adequate testosterone and estrogen levels to support that desire. This combination addresses both the “wanting” and the hormonal foundation simultaneously.
PT-141 + Oxytocin — Arousal + Connection: For researchers studying the intersection of desire and relational satisfaction, this combination pairs central arousal initiation with enhanced bonding and orgasmic function. PT-141 handles the drive component while oxytocin addresses the emotional and intimacy dimensions.
Kisspeptin + Pinealon — Hormonal Optimization: This stack targets the hormonal environment from two angles — Kisspeptin activates the HPG axis from the top while Pinealon removes circadian and stress-related suppression of that same axis. Particularly relevant for research into age-related or stress-induced hormonal decline.
Full Stack — PT-141 + Kisspeptin + Oxytocin + Pinealon: The comprehensive approach targeting central arousal, hormonal production, emotional bonding, and neuroendocrine support simultaneously. Each compound operates through independent receptor systems, minimizing mechanism-overlap side effect risk.
Dosage Guidelines and Safety for Sexual Health Peptides
Proper dosage and administration are critical for both safety and efficacy in peptide research. For complete preparation instructions, see our peptide dosage guide.
| Peptide | Typical Research Dose | Administration | Onset | Key Safety Notes |
|---|---|---|---|---|
| PT-141 | 1.75 mg | Subcutaneous injection | 30-60 min | Max 8 doses/month. Nausea common. Monitor blood pressure. |
| Kisspeptin-10 | 1.0 nmol/kg IV (clinical research) | IV or subcutaneous | 15-30 min | Short half-life. Pulsatile dosing may be required. |
| Oxytocin | 20-40 IU | Intranasal spray | 30-60 min | Effects on trust/social behavior require awareness. Avoid chronic high-dose use. |
| Pinealon | 10-20 mg | Intranasal or sublingual | Cumulative over days | Generally well-tolerated. Best taken in evening due to melatonin effects. |
General safety considerations for all sexual health peptides:
- All peptides listed here are research chemicals unless specifically noted (PT-141/Vyleesi has FDA approval for a specific indication in women)
- Start with the lowest effective dose in any research protocol
- Proper reconstitution and storage are essential — peptides degrade rapidly when handled incorrectly
- Individual response varies significantly; published doses are population averages
- Consult a qualified healthcare professional before considering any peptide compound
Frequently Asked Questions About Peptides for Libido
What is the best peptide for increasing libido?
PT-141 (bremelanotide) has the strongest clinical evidence for directly increasing sexual desire. It’s the only peptide with FDA approval for a sexual health indication (HSDD in premenopausal women under the brand name Vyleesi). It works through central brain mechanisms rather than blood flow, making it effective for both men and women who don’t respond to PDE5 inhibitors like Viagra or Cialis. Finding a quality PT-141 for sale with 3rd party testing in the US is critical as there are a number of vendors that don’t produce their actual data.
Can peptides help with erectile dysfunction?
Yes — through a different mechanism than conventional ED drugs. PT-141 produced erectile responses in clinical trials with men who had failed sildenafil, because it initiates arousal centrally (through the brain) rather than peripherally (through blood vessels). Kisspeptin may also support erectile function indirectly by optimizing testosterone levels through HPG axis activation. These are complementary approaches, not replacements for existing treatments.
Are sexual health peptides safe?
PT-141 has the most extensive safety data, having gone through full FDA Phase III clinical trials with 1,247 patients. The most common side effect is transient nausea (approximately 40% of subjects), typically resolving within 2 hours. Kisspeptin and oxytocin have been used in numerous clinical research studies with generally favorable safety profiles. However, all peptides except FDA-approved formulations remain research compounds, and long-term safety data is limited. Always consult a healthcare professional.
How fast do sexual health peptides work?
PT-141 typically shows effects within 30-60 minutes of subcutaneous injection, with effects lasting up to 24 hours. Oxytocin onset is similar at 30-60 minutes via intranasal administration. Kisspeptin acts rapidly on the HPG axis (LH response within 15-30 minutes) but its hormonal optimization effects build over repeated dosing. Pinealon works cumulatively over days to weeks as neuroendocrine balance improves.
What is the difference between PT-141 and Viagra?
They work through entirely different mechanisms. Viagra (sildenafil) is a PDE5 inhibitor that increases blood flow to erectile tissue by blocking the enzyme that breaks down cGMP. It works on plumbing — blood vessels. PT-141 is a melanocortin receptor agonist that activates sexual desire and arousal circuits in the brain. It works on drive — the central nervous system. This is why PT-141 can work in patients where Viagra fails, and why PT-141 is effective in women while PDE5 inhibitors are not.
Can women use peptides for sexual health?
PT-141 was specifically approved by the FDA for use in premenopausal women with HSDD — it is the only FDA-approved treatment that addresses sexual desire through central brain mechanisms in women. Kisspeptin research includes female subjects, with particular relevance to hypothalamic amenorrhea and fertility. Oxytocin research spans both sexes with robust data on female sexual response, orgasm intensity, and pair bonding.
Research Disclaimer: All peptides listed on this site are intended for laboratory research purposes only. They are not approved by the FDA for human use, diagnosis, treatment, or prevention of any condition. Vyleesi (bremelanotide) is an FDA-approved drug for a specific indication in women; the information here is presented for educational context only and does not represent medical advice. NoProp Peptides does not condone or encourage self-administration of research chemicals.